



Primary soft tissue chondroma of the anterior mediastinum: A case report and comprehensive literature review
- Authors:
- Published online on: September 9, 2025 https://doi.org/10.3892/etm.2025.12966
- Article Number: 216
-
Copyright: © Zhang et al. This is an open access article distributed under the terms of Creative Commons Attribution License.
Abstract
Introduction
Anterior mediastinal soft tissue chondromas are a rare subset of a broader category of soft tissue chondromas that arise from mature hyaline cartilage. Although these tumors are most commonly found in the extremities, they can occasionally occur in the mediastinum (1-3). A literature review conducted by Bansal et al (4) revealed that 96% of soft tissue chondromas occur in the extremities, with the majority of cases involving patients aged 30-60 years. The incidence rate is approximately equal between the sexes. These tumors are not attached to the cortex or periosteum of the adjacent bone, although they may originate from synovial tissue (4). Importantly, these generally benign tumors are often misdiagnosed due to their similarity in imaging characteristics to other more common anterior mediastinal masses (e.g., thymomas, teratomas and lymphomas) (5). Therefore, accurate diagnosis is critical for ensuring appropriate management, as the treatment approach for chondromas differs significantly from that taken for more aggressive or malignant mediastinal tumors (3,6). In this article, a rare case of chondroma located in the anterior mediastinum is presented. This case emphasizes the necessity of factoring in anterior mediastinal soft-tissue chondromas when differentiating calcified mediastinal masses. Comprehensive imaging assessment and histopathological analysis are crucial for an accurate diagnosis and appropriate management, thus preventing the overtreatment of benign lesions.
Case report
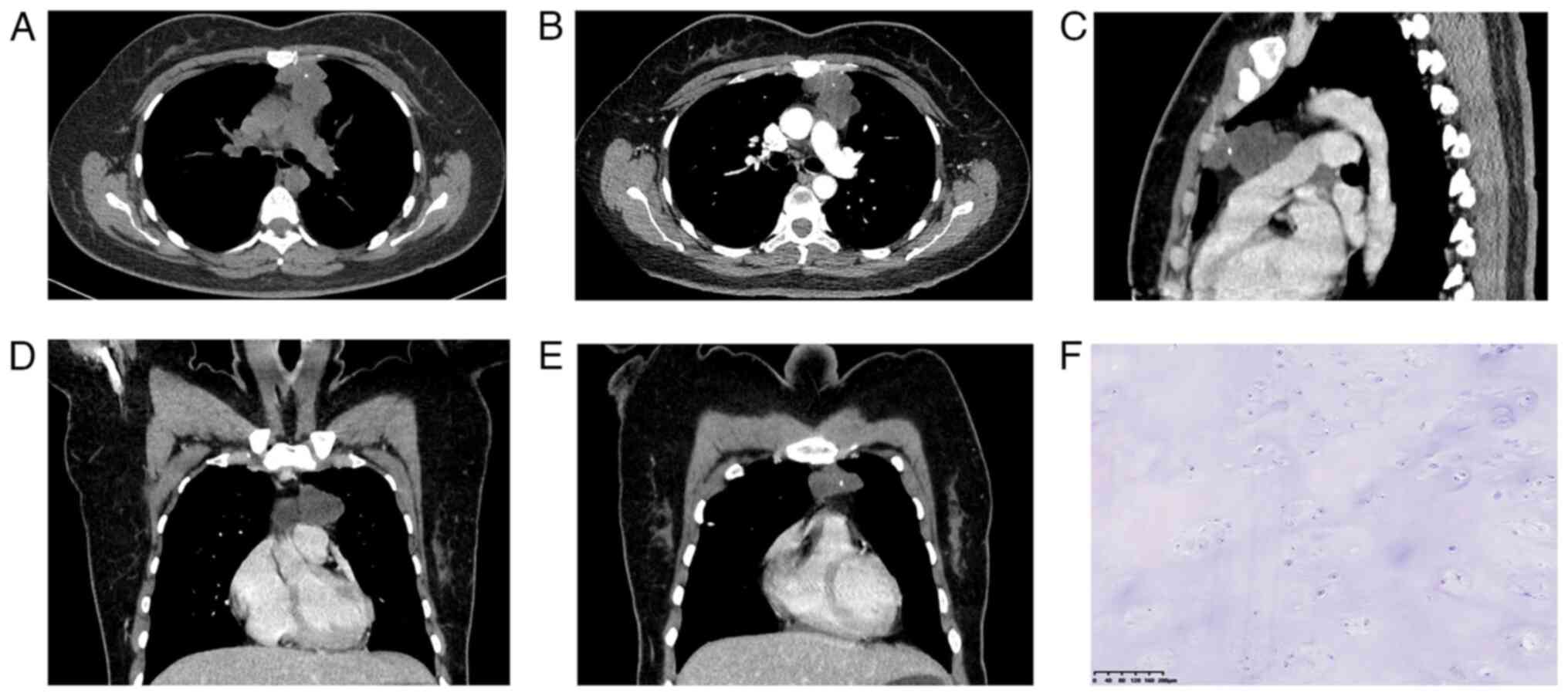
A 36-year-old Chinese female presented with an incidental finding of an anterior mediastinal mass during a routine health examination at a local hospital in June 2020. The patient was asymptomatic at the time of discovery, with no history of chest pain, dyspnea or other respiratory symptoms. Computed tomography (CT) revealed a lobulated, low-density mass measuring ~4.7x4.0 cm in the anterior mediastinum. Punctate calcifications were observed within the lesion and no significant enhancement was noted on contrast-enhanced imaging (Fig. 1A-E). The mass did not exhibit any signs of invasion into surrounding structures and there was no evidence of associated lymphadenopathy. Given the benign imaging characteristics, the patient underwent a median sternotomy for surgical resection of the mass. Intraoperatively, the tumor was well-encapsulated and easily separable from adjacent mediastinal structures (Fig. 1). The fully resected mass was confirmed the diagnosis of a soft tissue chondroma. The tumor was composed of mature hyaline cartilage with focal calcified areas and did not exhibit any signs of malignancy based on hematoxylin and eosin staining (Fig. 1F).
The postoperative recovery of the patient was uneventful and the patient was discharged in a stable condition. At the 6-month follow-up, the patient remained asymptomatic with no signs of recurrence on imaging examination, and further follow-up was arranged, but the patient was lost to follow-up.
Discussion
Chondromas can be classified into several types, including enchondroma, periosteal chondroma and multiple enchondromatosis. In addition to the aforementioned types, there is also a rare type known as soft tissue chondroma, also termed extraskeletal chondroma or chondroma of soft parts (7). Soft tissue chondroma represents a rare benign cartilaginous neoplasm pathognomonically defined by two exclusion criteria, namely absence of attachment to the bony cortex or periosteum and exclusion of intra-articular or tenosynovial localization (7). Soft tissue chondroma presents as a well-defined soft tissue mass and typically does not involve the underlying bone, though bone compression or erosion may occur. Plain radiographs often show characteristic ring-like or curvilinear calcifications (8). These tumors primarily affect the soft tissues of the hands and feet and, by definition, are not associated with synovial structures. Histologically, soft tissue chondromas exhibit lobulated growth patterns of mature hyaline cartilage, which are surrounded by fibrous tissue (9). In certain cases, they may show increased cellularity, myxoid changes and variable degrees of calcification (10). Accurate diagnosis can be challenging due to their rarity and nonspecific clinical presentation. In the present case, histopathological examination confirmed a diagnosis of soft tissue chondroma, a rare entity in the anterior mediastinum.
This case adds to the limited literature on mediastinal chondromas and underscores the importance of considering this differential diagnosis when encountering calcified mediastinal masses. A review of similar cases indicates that these rare tumors are generally well-circumscribed lesions and exhibit distinctive calcifications on imaging, which can aid in preoperative identification (2,5,11).
A summary of the literature was provided in Table I, which includes cases of soft tissue chondroma located in the mediastinum, as reported in English-language publications available on PubMed (https://pubmed.ncbi.nlm.nih.gov/). All of these studies involved a CT workup. Imaging, particularly CT, is essential for the diagnosis of mediastinal soft tissue chondromas (2,5,12). These tumors often appear as well-circumscribed masses with areas of calcification (a hallmark imaging feature). Fang et al (2) documented a case of a posterior mediastinal soft tissue chondroma characterized by a well-circumscribed, calcified mass with no significant enhancement on imaging (a common feature of benign soft tissue tumors) Similarly, Shrivastava et al (5) highlighted the use of CT in identifying a benign soft tissue chondroma in a 37-year-old female with a well-circumscribed, calcified mass in the anterior mediastinum. Additionally, Widdowson and Lewis-Jones (12) reported a large soft tissue chondroma in the posterior mediastinum with extensive, irregular calcifications and a well-defined border, without attachment to adjacent ribs or the spine. This case report further supported the utility of CT in differentiating these lesions from other mediastinal tumors. Based on the three previously reported cases and the present case, the CT manifestations of mediastinal chondroma may be summarized as follows. Firstly, a round or oval mass occurs in the anterior or posterior mediastinum, which may be lobulated. Secondly, well-defined margins are present. Thirdly, focal, linear, curvilinear or other irregular calcifications may be observed within the mass. Finally, no enhancement or minimal enhancement is observed on enhanced CT. In addition to mediastinal chondroma, other mediastinal masses may also present with calcification. Therefore, a differential diagnosis is required when encountering a mediastinal mass with calcified features on clinical imaging. The differential diagnosis includes thymomas, teratomas and chondrosarcomas; though these masses may present with similar imaging findings, they are treated with completely different therapeutic regimens and associated with varied prognoses (12). Calcified mediastinal tumors represent a diagnostic challenge, with various benign and malignant entities displaying distinct patterns of calcification. Common tumors with calcifications include thymomas, teratomas and post-radiation lymphomas. Thymomas often exhibit linear or septal calcifications, particularly in cases of advanced disease, while teratomas present with coarse calcifications associated with fat, bones or teeth. Calcifications in lymphomas are rare and typically occur post irradiation. Other entities, such as pericardial cysts, intrathoracic goiters and neurogenic tumors, may also present with calcifications, although less frequently. CT imaging plays a pivotal role in identifying calcifications and differentiating these tumors, while magnetic resonance imaging aids in further soft tissue characterization (13-15). This case highlights the critical role of imaging in the diagnosis and management of mediastinal chondromas. Furthermore, it underscores the importance of histopathological confirmation in ensuring accurate diagnosis and appropriate treatment.
The present study has its limitations, which are worth mentioning. The absence of iodine density maps may have affected the in-depth analysis of relevant factors, thus limiting the comprehensiveness of the research results.
In conclusion, anterior mediastinal soft tissue chondroma is a rare tumor type. It is characterized by a well-defined, calcified lesion with possible slight enhancement. When encountering a mediastinal tumor with calcification, it is important to consider chondroma in the differential diagnosis. Accurate diagnosis through a combination of imaging and histopathology is essential for guiding appropriate surgical management and ensuring favorable patient outcomes. This case report contributes to the limited literature on anterior mediastinal chondromas and underscores the importance of clinical vigilance and comprehensive diagnostic evaluation in managing these rare tumors.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
YZ and MP served as the principal investigators, making substantial contributions to the study design, developing the treatment plan and overseeing the analysis and interpretation of the patient's clinical data. YZ also participated in the drafting and revision of the manuscript and approved the final version. XG designed the case study, contributed to clinical decision-making and assisted with manuscript revision. MZ and CL were responsible for acquiring key medical images and confirmed the authenticity of all raw data. All authors have read and approved the final manuscript.
Ethics approval and consent to participate
This study was conducted in accordance with the principles expressed in the Declaration of Helsinki.
Patient consent for publication
The patient provided written informed consent for the publication of this case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
References
|
Marcial-Seoane RA, Marcial-Seoane MA, Ramos E and Marcial-Rojas RA: Extraskeletal chondromas. Bol Asoc Med P R. 82:394–402. 1990.PubMed/NCBI | |
|
Fang S, Liu L, Zhang M, Pan N, Gao W, Pan J and Liu J: Primary soft tissue chondroma of the posterior mediastinum: A rare case report and literature review. J Int Med Res. 49(3000605211053557)2021.PubMed/NCBI View Article : Google Scholar | |
|
Benradi L, El Haissoufi K, Haloui A, Bennani A, Aichouni N and Belahcen M: Soft tissue chondroma of the plantar foot in a 14-year-old boy: A case report. Int J Surg Case Rep. 90(106688)2022.PubMed/NCBI View Article : Google Scholar | |
|
Bansal M, Goldman AB, DiCarlo EF and McCormack R: Soft tissue chondromas: Diagnosis and differential diagnosis. Skeletal Radiol. 22:309–315. 1993.PubMed/NCBI View Article : Google Scholar | |
|
Shrivastava V, Vundavalli S, Smith D and Tennant D: A chondroma of the anterior mediastinum. Clin Radiol. 61:1065–1066. 2006.PubMed/NCBI View Article : Google Scholar | |
|
Zlatkin MB, Lander PH, Begin LR and Hadjipavlou A: Soft-tissue chondromas. AJR Am J Roentgenol. 144:1263–1267. 1985.PubMed/NCBI View Article : Google Scholar | |
|
Uhl M, Herget G and Kurz P: Cartilage tumors: Pathology and radiomorphology. Radiologe. 56:476–488. 2016.PubMed/NCBI View Article : Google Scholar : (In German). | |
|
Hondar Wu HT, Chen W, Lee O and Chang CY: Imaging and pathological correlation of soft-tissue chondroma: A serial five-case study and literature review. Clin Imaging. 30:32–36. 2006.PubMed/NCBI View Article : Google Scholar | |
|
Gentles C, Perin J, Berrey H and Griffiths HJ: Soft-tissue chondroma. Orthopedics. 30:180, 241-183. 2007.PubMed/NCBI View Article : Google Scholar | |
|
Kao YC, Lee JC and Huang HY: What is new about the molecular genetics in matrix-producing soft tissue tumors? -The contributions to pathogenetic understanding and diagnostic classification. Virchows Arch. 476:121–134. 2020.PubMed/NCBI View Article : Google Scholar | |
|
Somers J and Faber LP: Chondroma and chondrosarcoma. Semin Thorac Cardiovasc Surg. 11:270–277. 1999.PubMed/NCBI View Article : Google Scholar | |
|
Widdowson DJ and Lewis-Jones HG: A large soft-tissue chondroma arising from the posterior mediastinum. Clin Radiol. 39:333–335. 1988.PubMed/NCBI View Article : Google Scholar | |
|
Yokota K, Sakamoto A, Matsumoto Y, Matsuda S, Harimaya K, Oda Y and Iwamoto Y: Clinical outcome for patients with dedifferentiated chondrosarcoma: A report of 9 cases at a single institute. J Orthop Surg Res. 7(38)2012.PubMed/NCBI View Article : Google Scholar | |
|
Hodler J, Kubik-Huch RA and von Schulthess GK: Diagnostic and Interventional Imaging. In: Diseases of the Chest, Breast, Heart and Vessels 2019-2022: IDKD Springer Series, 2019. | |
|
Ahuja J, Strange CD, Agrawal R, Erasmus LT and Truong MT: Approach to imaging of mediastinal masses. Diagnostics (Basel). 13(3171)2023.PubMed/NCBI View Article : Google Scholar |










